Tuberculosis

Recently, SphereMD has had several active Tuberculosis (TB) cases from mariners entering the U.S. In each case, the patient had advanced active disease with significant respiratory symptoms. These cases all required extended hospitalizations, high expense, and, in one circumstance, a very complicated repatriation.
TB History & Risk:
Life and work aboard a merchant ship is characterized by crowded, enclosed spaces. The crews of ships are often multinational, coming from countries identified by the CDC as having a “high burden” of TB. This list includes Bangladesh, India, Indonesia, Myanmar, Philippines, China, Brazil, and several other countries. This combination of sustained proximity and populations with increased incidence of TB is a serious potential health threat to mariners and a risk management issue for vessel owners.
TB is a bacterial infection transmitted by respiratory droplets from an infected individual. There are multiple risk factors for TB, including proximity and duration of exposure to an infected individual and the severity of the infected individual’s TB infection. Several factors have resulted in resistance to the drugs used to treat TB. Some strains of TB may also be multi-drug resistant or extensively drug resistant.
TB Infection:
TB infection has three stages: primary infection, latent or dormant infection, and active infection. The incubation period for infection of TB is 2-12 weeks, with the risk of developing active disease highest within the first two years of infection.
It is important to note that only 1 in 10 people who have latent TB will develop active TB.
Most patients with TB can be successfully treated. However, patients with some types of extensively drug-resistant TB have a mortality rate at or above 50%
Suspected TB in a Mariner:
Once TB infection is suspected in a mariner in the U.S., the mariner’s medical care becomes dictated by public health concern and U.S. law. Upon suspicion of TB, doctors will order that the patient be hospitalized and transferred to a negative flow isolation room under respiratory precautions. This means that regardless of the actual acuity or level of patient illness, the patient will be placed in a private room in a “high” care medical setting.
Post-isolation, the patient will undergo a battery of tests that may include X-ray, CT Scan, laboratory studies, and sputum cultures. The patient also may be preemptively started on antibiotics while test results are pending.
Before a patient with suspected TB is discharged from the hospital they must have three negative sputum cultures. Since sputum cultures generally take 72 hours to grow, minimum hospitalization time is generally seven days just to rule out the presence of TB.
Further, in some circumstances, physicians may keep patients in the hospital even in the absence of positive sputum cultures. The bottom line is that suspicion of TB by a U.S. physician usually means a minimum of one week hospitalization and associated expenses.
Treating TB in a Mariner:
Once TB is diagnosed by a sputum culture, the lab sends the culture out to determine which drugs the patient’s specific TB is “sensitive” to. Assuming the patient has nondrug-resistant TB, the conventional therapy is started to treat the infection. If the patient has drug-resistant TB, multiple sputum samples will be sent to the lab in search of drugs that are effective for the patient’s strain of TB.
U.S. law requires that the hospital inform the State Health Department of the patient’s infection in whichever state the patient is receiving care. The State Health Department is then responsible for informing the U.S. CDC of the infection in specific circumstances. Once the case is confirmed, the state and/or CDC must be consulted and approve both treatment and discharge from the hospital.
The length of treatment will vary depending on several factors including drug resistance, the patient’s overall health, and the degree of infection at admission. Practically speaking, patients can be discharged after three negative sputum cultures in as little as two weeks. For patients with extensive disease, or any form of drug-resistant TB, hospitalizations may last months.
SphereMD has had two cases in the last 90 days with hospitalizations lasting over 60 days. Of these cases, one patient had extensively drug-resistant TB and required a chartered jet to repatriate; the other had a non-drug-resistant TB with very concentrated disease in his lungs.
TB Treatment Differences forNon-Mariners:
Most non-drug-resistant TB patients who are U.S. residents would be discharged home after diagnosis and stabilization, usually within a couple of weeks. Precautions would be taken to protect the patient’s family members from acquiring TB. The patient would be ordered to avoid contact with people outside of the home. Treatment would be monitored by the State Health Department to assure compliance with the treatment regimen. Monitoring would include regular sputum cultures, examinations, and possibly home visits by a public health nurse.
Repatriation:
As previously mentioned, TB patients who are mariners are not usually allowed to leave isolated hospital rooms until they have produced three negative sputum cultures confirming that they are no longer infected with active TB. Once this has occurred, patients may fly aboard commercial flights without special precautions.
In certain circumstances, it is possible to repatriate a patient with active TB who is stable and for whom extended treatment is anticipated. Because such patients are public health risks, these repatriations become quite complicated. In the most extreme cases, these patients will require a repatriation plan that is approved by the State Health Department, the CDC, and the WHO. A qualified, approved physician must be found in the patient’s home country who will continue the patient’s care upon repatriation. Because of the public health risk, the patient will likely require repatriation by air ambulance. For patients with extensively drug-resistant TB, few air ambulance companies will transport these patients. Air ambulance costs for these patients are high. We have seen quotes ranging from $163,000.00 USD to $365,000.00; the latter amount was for an aircraft equipped to transport Ebola patients.
Follow Up for Crew Who Were Exposed:
It is vitally important that crewmembers who have been exposed to a patient with active TB be screened for TB. Upon determination that they were exposed to active TB, all crewmembers, including those who have signed off, should receive initial screening with a blood test called a QuantiFERON-TB Gold (QFT). Eight to ten weeks later, the exposed crewmembers will require a second QFT test. It should be noted that TB skin tests are not appropriate for non-U.S. born crewman. X-rays are not effective as they will not show latent TB and are only useful for ruling out active TB. It is also important to remember that with the multinational population of ship crews, it is likely that some of the crew will have a positive QFT. Crewmen with a positive QFT will require a chest X-Ray to rule out active TB.
The public health officer who is charged with the crewman’s care should be the individual charged with making screening recommendations for the patient’s contacts.
Screening:
Of the recent TB cases described above, all the patients had advanced symptomatic infection. While most manning companies require screening for TB, the advanced disease seen in these patients causes some concern about the effectiveness of this screening.
Examining the Costs of a U.S. TB case:
Costs shown below are from a simple TB case treated in 2015. The crewman was hospitalized for only 16 days.
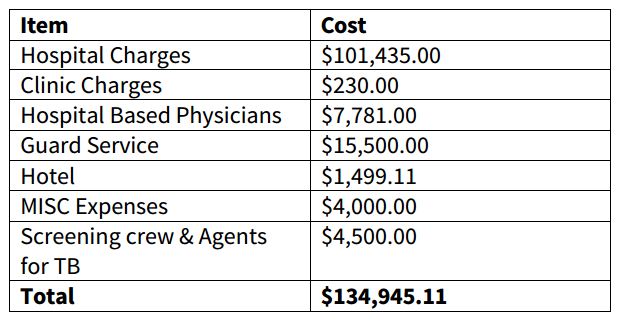
It is important to note that there were additional costs associated with this case that are not detailed above including legal fees, medical management, and any supplementary crew claims. Further, this patient had a 16-day hospitalization and responded to treatment quickly. Imagine the extensive costs with a 30-, 60-, or 90-day hospitalization.
Summary:
TB is a public health issue that poses a serious health and financial risk to ship owners and their crews. Pre-employment screening for TB in ship crews may be ineffective. Once TB is suspected by a U.S. physician, treatment will likely extend for a minimum of 10 days and may continue for many months. With the minimum cost of the simplest 10-day hospitalization being $10,000.00-$20,000.00 USD, TB treatment in the U.S. is a huge potential expense. Unlike other medical issues, most TB patients cannot be repatriated for treatment. Because TB is a serious public health issue, all crewmembers who have been in contact with the infected patient, including those who have signed off, must be screened at least twice for TB.
TB treatment in the U.S. may be confusing to ship owners for several reasons. First, the crewman is sometimes required to stay in the hospital for no other reason than to assure that they are compliant with the medication regimen and that they do not make contact with the U.S. population. Expensive guard service is often required even though the patient is hospitalized. There is also little predictability about how fast or effective treatment may be, so the length of the hospitalization is uncertain, and crew managers often feel an understandable lack of control. Further, requirements for screening all crewmembers who have had sustained contact with the infected patient is financially burdensome and logistically difficult. Finally, the U.S. health authorities tend to be inflexible about treatment regimens, citing public health concerns.
Recommendations:
- SphereMD recommends that all companies evaluate their pre-employment TB screening programs for effectiveness.
- Contact your P&I Club immediately should a diagnosis of TB be suspected or confirmed.
- In the event of a TB exposure, quickly and effectively screen exposed crewmembers using the previously stated methods.